Views: 0 Author: Site Editor Publish Time: 2025-12-19 Origin: Site
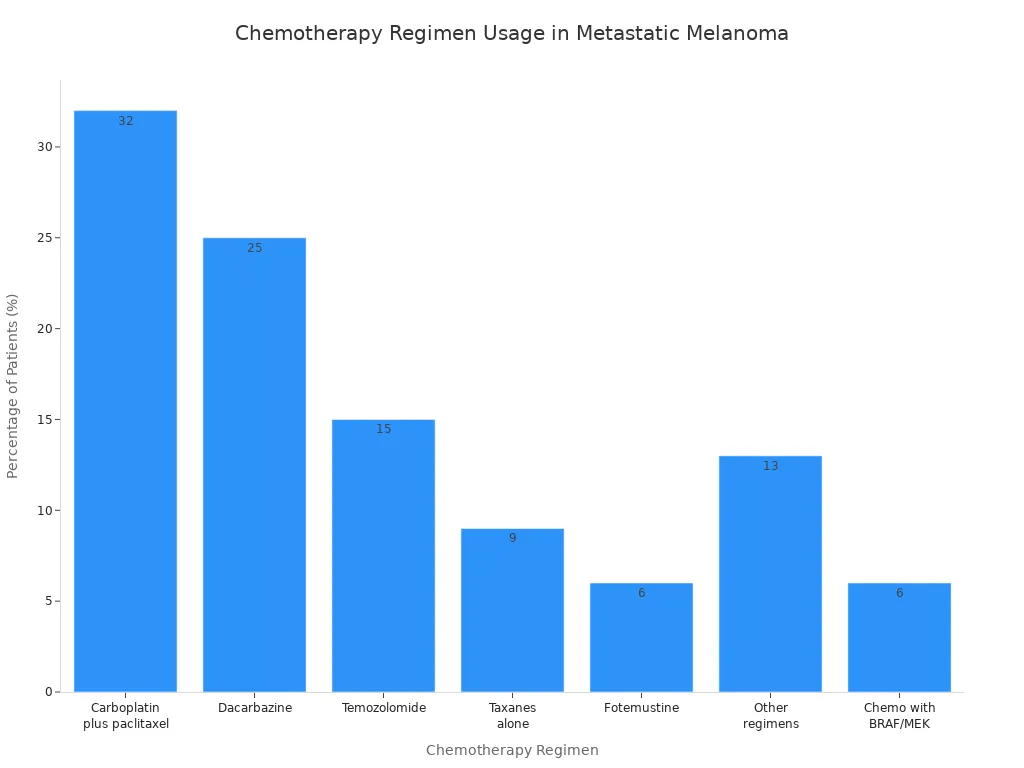
Chemotherapy Regimen | Percentage (%) |
|---|---|
Carboplatin plus paclitaxel | 32 |
Dacarbazine | 25 |
Temozolomide | 15 |
Taxanes alone | 9 |
Fotemustine | 6 |
Other regimens | 13 |
Chemotherapy with BRAF/MEK therapy | 6 |
You might feel scared about starting chemotherapy. You are not the only one. Chemotherapy drugs still help treat metastatic melanoma. They are used when other treatments do not work.
Chemotherapy drugs like dacarbazine and carboplatin help treat metastatic melanoma when other treatments do not work.
Knowing how chemotherapy drugs work can help you talk with your doctor about your treatment choices.
You should know about side effects from chemotherapy, like feeling very tired and losing hair, and tell your healthcare team if you have any worries.
You can think about joining clinical trials to try new treatments that might help with metastatic melanoma.
Always ask your doctor what treatment is best for you, and if you can use more than one therapy.
Chemotherapy drugs for metastatic melanoma are made very carefully. Every step is important for your safety and for the drugs to work well.
Many advanced machines help make chemotherapy drugs. Each one does a special job:
Vial Filling Sealing Line: This machine puts liquid drugs in glass vials and seals them tight.
Prefilled Syringe Filling Line: It gets syringes ready with the right amount of medicine.
Cartridge Filling Line: This fills cartridges that doctors use for some shots.
Ampoule Filling Sealing Line: It puts medicine in small glass ampoules and seals them for one-time use.
Oral Liquid Filling Line: This machine fills bottles with liquid drugs you can drink.
Syrup Filling Line: It works like the oral liquid line but for thicker medicine.
Blow-Fill-Seal (BFS) Machine: This machine makes, fills, and seals containers in one step to keep drugs clean.
Isolator System: It makes a closed, clean space to keep germs away from the drugs.
Pharmaceutical Liquid Preparation System: This mixes and gets the drug solutions ready.
Pharmaceutical Water Treatment System: It cleans the water used to make the drugs.
Other Pharmaceutical Machines: These are mixers, mills, and machines that put labels on.
Tip: All these machines help keep the drugs clean and safe for you.
You want your chemotherapy drugs to be safe and work well. Makers follow strict rules to make sure of this. The FDA and EMA check and approve every drug. Good Manufacturing Practices (GMP) guide each step. Workers test the starting materials, mixtures, and finished drugs many times. They use trusted suppliers and check everything for quality.
A risk assessment helps find and fix problems before you get the drugs. Teams keep making the process better to make drugs safer over time. Sterilization machines, like autoclaves and isolators, kill germs and keep you healthy.
Note: Quality control means you get medicine that works right every time.
If you have metastatic melanoma, you will learn about different chemotherapy drugs. Each drug fights melanoma in its own way. You should know how these drugs work on cancer cells. This helps you understand your treatment.
Alkylating agents are some of the oldest chemotherapy drugs for melanoma. These drugs attack the DNA inside melanoma cells. Damaged DNA stops cells from dividing or growing. This helps stop metastatic melanoma from spreading.
Dacarbazine is the most common alkylating agent for metastatic melanoma. Doctors pick this drug because it slows melanoma growth. You might also hear about temozolomide and lomustine. These drugs work in a similar way.
Note: Alkylating agents can help when other treatments do not work for metastatic melanoma.
Here is a table that shows how dacarbazine helps patients with metastatic melanoma:
Alkylating Agent | Study Type | Patient Group | Progression-Free Survival (PFS) | Overall Survival (OS) |
|---|---|---|---|---|
Dacarbazine (+/− Oblimersen) | Phase III (n=771) | Normal serum LDH | 2.6 months | 11.4 months vs 9.7 months |
Dacarbazine gives patients more time before their melanoma gets worse.
Platinum-based agents are another group of chemotherapy drugs for metastatic melanoma. These drugs have platinum, which is a metal. The drugs stick to DNA in melanoma cells. This stops cells from copying DNA. When cells cannot copy DNA, they die.
Cisplatin and carboplatin are the main platinum-based drugs for metastatic melanoma. Doctors use these drugs alone or with other chemotherapy drugs. Platinum-based agents can shrink tumors and help control symptoms.
Tip: Platinum-based agents are strong drugs. You may need extra care to handle side effects.
Microtubule inhibitors are special chemotherapy drugs. They target microtubules inside melanoma cells. Microtubules help cells divide. When these drugs block microtubules, cells cannot split or grow.
You might get paclitaxel, docetaxel, vinblastine, or vincristine for metastatic melanoma. Paclitaxel and docetaxel make microtubules too stable. Vinblastine and vincristine stop microtubules from forming. Both ways, these drugs stop melanoma cells from spreading.
Here is a table that shows how these drugs work:
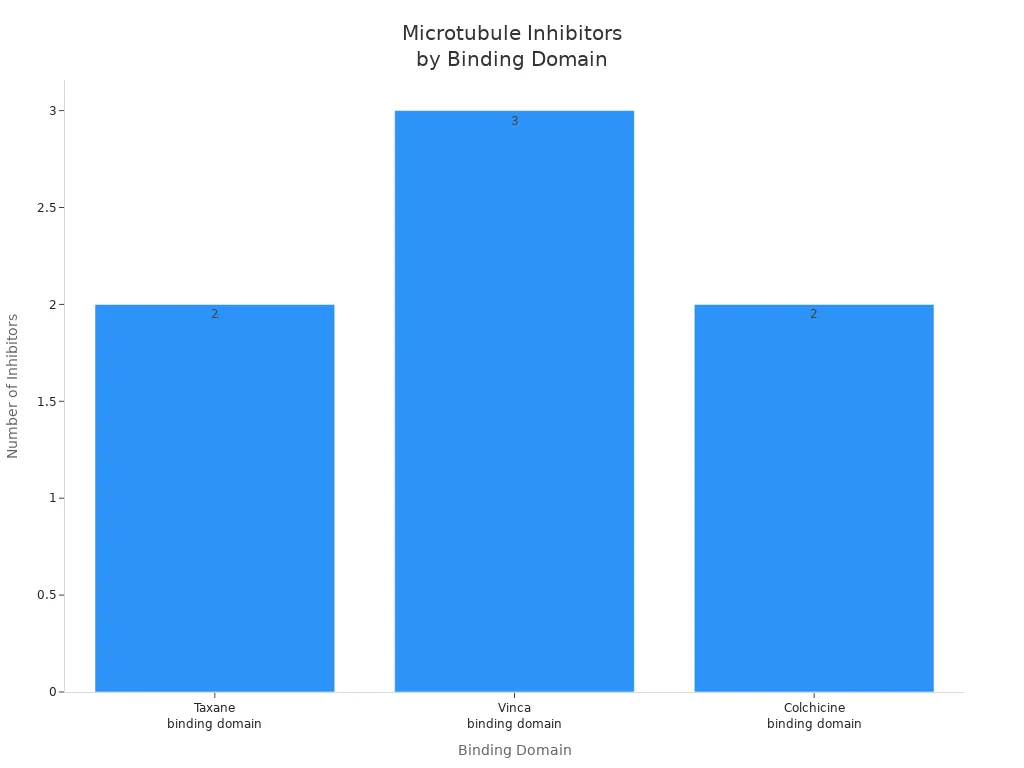
Microtubule Inhibitor | Mechanism of Action | Binding Domain |
|---|---|---|
Paclitaxel (PTX) | Promotes tubulin polymerization, causing cell cycle arrest | Taxane binding domain |
Docetaxel (DTX) | Promotes tubulin polymerization, causing cell cycle arrest | Taxane binding domain |
Vinblastine | Inhibits microtubule polymerization | Vinca binding domain |
Vincristine | Inhibits microtubule polymerization | Vinca binding domain |
Vinorelbine | Inhibits microtubule polymerization | Vinca binding domain |
Combretastatin (CA) | Inhibits microtubule polymerization | Colchicine binding domain |
Colchicine | Inhibits microtubule polymerization | Colchicine binding domain |
Paclitaxel has helped some patients with untreated metastatic melanoma. Some people saw their lung tumors shrink for almost a year.
Microtubule inhibitors give you more choices if other chemotherapy drugs do not work for your melanoma.
Antitumor antibiotics are a special group of chemotherapy drugs. These drugs come from natural sources like bacteria. They block enzymes that melanoma cells need to copy DNA. If cells cannot copy DNA, they cannot grow.
Actinomycin D is one example. Doctors do not use this drug often for metastatic melanoma because it can cause more side effects. Sometimes doctors use it in special cases.
Alert: Antitumor antibiotics are very strong. Your doctor will watch you closely if you get these drugs for metastatic melanoma.
You will hear many names when you talk about chemotherapy for metastatic melanoma. Some drugs are used alone. Others are mixed together in regimens. Regimens are plans that use different drugs to fight melanoma in more than one way.
Here is a table with common chemotherapy drugs and their classes:
Drug Name | Drug Class | Main Use in Melanoma |
|---|---|---|
Dacarbazine | Alkylating Agent | Standard for metastatic melanoma |
Temozolomide | Alkylating Agent | Oral option for metastatic melanoma |
Cisplatin | Platinum-Based Agent | Used in combinations |
Carboplatin | Platinum-Based Agent | Used in combinations |
Paclitaxel | Microtubule Inhibitor | Used in regimens |
Vinblastine | Microtubule Inhibitor | Used in regimens |
Actinomycin D | Antitumor Antibiotic | Rarely used |
Doctors often use regimens like:
Carboplatin plus paclitaxel: This is a common choice for metastatic melanoma.
Dacarbazine alone: Used when you need a single drug.
BOLD regimen: Combines bleomycin, vincristine, lomustine, and dacarbazine.
CVD regimen: Uses cisplatin, vinblastine, and dacarbazine.
Dartmouth regimen: Mixes cisplatin, carmustine, dacarbazine, and tamoxifen.
Your doctor will pick the best regimen for your melanoma based on your health and how your metastatic melanoma responds to treatment.
Chemotherapy drugs give you many ways to fight metastatic melanoma. Each drug and regimen has a special job. You and your doctor can work together to find the best plan for your melanoma.
Chemotherapy drugs fight melanoma in different ways. Each drug stops cancer cells from growing or spreading.
Some chemotherapy drugs stop melanoma cells from splitting. These drugs target the cell cycle. The cell cycle is how cells grow and multiply. Paclitaxel and doxorubicin slow down melanoma cell growth. They work based on how much and how long you use them. Some drugs work better together. The table below shows how these treatments change cell growth:
Treatment Type | Effect on Cell Growth | Correlation with CDC25A mRNA Level |
|---|---|---|
Doxorubicin | Inhibited growth in a dose- and time-dependent manner | Negatively correlated |
Paclitaxel | Inhibited growth in a dose- and time-dependent manner | Not correlated |
Combination with NSC663284 | Lower cell viability compared to control or single-drug groups | N/A |
These drugs keep melanoma cells from finishing division. This slows down how fast melanoma spreads.
Some chemotherapy drugs make melanoma cells die. This is called apoptosis. Cisplatin causes damage that cells cannot fix. When this happens, cells stop working or break apart. Here are ways chemotherapy drugs cause cell death:
Cisplatin makes DNA damage. This leads to cell death or stops cell growth.
5-fluorouracil blocks an enzyme called thymidylate synthase. This causes DNA damage and stops the cell cycle.
Some melanoma cells resist these drugs. Researchers look for new ways to make cells die, like necroptosis.
These drugs help shrink melanoma tumors. They do this by killing cancer cells.
Chemotherapy drugs can stop melanoma cells from copying DNA. Without new DNA, cells cannot make new cells. Different drugs use different tricks to block DNA copying. The table below shows how these drugs work:
Mechanism | Description |
|---|---|
DNA Damage | Alkylating agents cause DNA damage, leading to melanoma cell death. |
Methylation Modifications | Methylating drugs create mismatches during DNA copying, causing breaks. |
Crosslinking | Some drugs link DNA strands together, stopping replication and transcription. |
Here is another table that shows how certain drugs block DNA copying:
Drug | Mechanism | Effect |
|---|---|---|
5-Fluorouracil | Inhibits thymidylate synthase | Reduces building blocks for DNA, blocking replication. |
Gemcitabine | Targets ribonucleic acid reductase | Stops cells from making new DNA. |
Cisplatin | Forms DNA crosslinks | Blocks DNA copying, leading to cell death. |
These drugs stop melanoma cells from making more copies. This helps control melanoma growth in your body.
If you know how chemotherapy drugs work, you may feel better about your treatment plan.
When you have metastatic melanoma, you want to know if chemotherapy helps. You also want to see how it compares to other treatments. This section explains how well chemotherapy, immunotherapy, and targeted therapy work. You will learn about response rates and survival outcomes. You will also find out how new drugs and clinical trials change treatment for metastatic melanoma.
Your doctor may talk about response rate. This means how many people see their tumor shrink or stop growing after treatment. In metastatic melanoma, chemotherapy does not work for most people. Clinical trials show only a few patients see their tumors shrink with chemotherapy drugs. Dacarbazine is a main drug. It has a response rate of about 10% to 20%. So, out of 100 people, only 10 to 20 see their tumor get smaller after chemotherapy.
You might get chemotherapy if your melanoma spreads far or if other treatments do not help. Doctors use clinical trials to test new drugs and combinations. Some trials mix chemotherapy with other drugs to try to help more people. The BOLD regimen and CVD regimen use several drugs to fight melanoma cells in different ways. These regimens sometimes help more people in trials, but the benefit does not last long for most.
You may hear about progression-free survival. This means how long you live without your melanoma getting worse. Chemotherapy drugs for metastatic melanoma usually give a short progression-free survival. Most people see their tumors grow again after a few months. Clinical trials show that overall survival with chemotherapy is limited. You may get a few extra months, but the tumor often comes back.
If you join a clinical trial, you may get new drugs that could help more. Ask your doctor about clinical trials for metastatic melanoma.
You have more choices for treating metastatic melanoma now. Immunotherapy and targeted therapy changed how doctors treat melanoma that spreads. These treatments work better for many people, especially if you have a BRAF mutation.
Look at the table below. It shows the two-year overall survival rate for different treatment orders in metastatic melanoma:
Treatment Order | Two-Year Overall Survival Rate |
|---|---|
Immunotherapy first | 72% |
Targeted Therapy first | 52% |
If you get immunotherapy first, you have a better chance to live two years or more. Targeted therapy also helps, especially if your melanoma has a BRAF mutation. Chemotherapy does not give the same survival benefit.
Here is another table that compares overall survival rate and progression-free survival rate for each treatment:
Treatment Type | Overall Survival Rate | Progression-Free Survival Rate |
|---|---|---|
Immunotherapy | 72% | Trending favorably |
Targeted Therapy | 52% | N/A |
Immunotherapy gives you the best chance for long-term survival. Targeted therapy also helps if you have the right mutation. Chemotherapy gives limited overall survival and does not improve progression-free survival for most people with metastatic melanoma.
You can see the clinical benefits of each treatment in the table below:
Treatment Type | Overall Survival Benefit | Progression-Free Survival Benefit |
|---|---|---|
Chemotherapy | Limited | No improvement |
Immunotherapy | Significant improvement | Significant improvement |
Targeted Therapy | N/A | N/A |
You may get chemotherapy if you cannot use immunotherapy or targeted therapy. Some people with rare mutations or special types of metastases may still need chemotherapy. Clinical trials keep testing new drugs to help treat metastatic melanoma.
Talk to your doctor about the best treatment for your melanoma. Ask about your BRAF mutation status, the type of metastases you have, and if you can join clinical trials for new drugs.
You have many choices for treating metastatic melanoma. Immunotherapy and targeted therapy give better survival and response rates for most people. Chemotherapy still helps some, especially if other treatments do not work. New drugs and clinical trials bring hope for better results and longer survival in the future.
When you begin treatment for melanoma, you will learn about different ways to get chemotherapy. Each way has good points and some problems. Your doctor picks the best way for you. This depends on your health and the kind of melanoma you have.
Doctors often use intravenous (IV) methods for melanoma. You get medicine through a needle or tube in your vein. The drugs go into your blood fast and start fighting melanoma cells. Nurses watch you closely during IV treatment. You may sit in a special chair at the hospital or clinic. IV methods help many types of melanoma, especially when the cancer has spread.
Some people with melanoma take chemotherapy as pills or capsules. You can swallow these drugs at home. Oral chemotherapy lets you stay comfortable and free. You do not need to go to the hospital as much. But your body may take in the medicine differently each time. You must remember to take your medicine on time. Missing doses can make melanoma harder to treat.
Chemotherapy for melanoma usually follows a cycle. You take the drugs for a set number of days, then rest. This pattern helps your body recover between treatments. Your doctor will tell you how many cycles you need. The number depends on how your melanoma responds. You may feel tired or have other side effects during each cycle. Common side effects are fatigue, hair loss, nausea, vomiting, low blood count, mouth sores, and skin rash.
Here is a table that shows the main ways to get chemotherapy for melanoma:
Method of Administration | Advantages | Disadvantages |
|---|---|---|
Intravenous (IV) | Rapid delivery to the bloodstream | Requires medical supervision |
Oral | Convenient and can be taken at home | Variable absorption rates |
Combination Therapy | Increases effectiveness against cancer cells | Higher risk of side effects |
Tip: Always talk to your doctor if you have questions about your melanoma treatment plan.
When you get chemotherapy for melanoma, your body may change. These drugs fight melanoma cells, but they can hurt healthy cells too. You might feel tired or weak. Some people lose hair or feel sick. Others get mouth sores or nail changes. Your skin may get dry or itchy. You could bruise or bleed more because your blood cell count drops.
Doctors watch for side effects to keep you safe. The table below lists common problems people have during melanoma treatment:
Chemotherapy Drug | Common Grade 3/4 Adverse Events |
|---|---|
General | Neutropenia, Vomiting, Anemia |
Vemurafenib | Cutaneous squamous-cell carcinoma, Rash, Elevated liver enzymes |
Dabrafenib | Cutaneous squamous-cell carcinoma, Pyrexia |
Trametinib | Hypertension, Rash |
Ipilimumab | Immune-related diarrhea/colitis, Dyspnea, Anemia, Vomiting, Hypophysitis |
Talimogene laherparepvec | Cellulitis |
You may feel numbness in your hands or feet. Some people notice changes in vision or hearing. Always tell your doctor about new symptoms. Your safety is very important during melanoma treatment.
You can do things to help with side effects from chemotherapy. Drink lots of water to help your body. Eat small meals if you feel sick. Rest when you are tired. Use gentle shampoo if you lose hair. Wear sunscreen to protect your skin, since melanoma and its treatment can make you more sensitive to sunlight.
Doctors may give you medicine for nausea or to help you sleep. Nurses check your blood often to keep you safe. If you get a fever or chills, call your doctor right away. Quick action helps keep you safe.
Tip: Write down your symptoms in a diary. This helps your care team change your melanoma treatment for better safety and comfort.
You help keep yourself safe. Stay in touch with your care team and ask questions about your melanoma treatment. By working together, you can handle side effects and focus on getting better.
You might wonder when doctors use chemotherapy drugs for metastatic melanoma. Most people start with immunotherapy or targeted therapy. These treatments help many patients. If these do not work, your doctor may suggest chemotherapy. Sometimes, you cannot get immunotherapy or targeted therapy because of other health issues. In those cases, chemotherapy is important.
Doctors check your melanoma type and your health before making a plan. If you have a BRAF mutation, you may get targeted therapy first. If you do not have this mutation, immunotherapy is usually the first choice. Chemotherapy is used when other treatments do not help or if your melanoma grows fast.
Here is a table that shows common treatment choices for different types of metastatic melanoma:
Patient Type | Recommended Treatments |
|---|---|
BRAF Wild-Type, Unresectable/Metastatic Melanoma | Nivolumab + Ipilimumab, Nivolumab + Relatlimab, Nivolumab, Pembrolizumab |
BRAF Mutant (V600), Unresectable/Metastatic Melanoma | Nivolumab + Ipilimumab, Nivolumab + Relatlimab, Nivolumab, Pembrolizumab, Dabrafenib + Trametinib, Encorafenib + Binimetinib, Vemurafenib + Cobimetinib |
New Recommendation (2023) | Nivolumab + Relatlimab based on RELATIVITY-047 trial results |
Doctors use chemotherapy for metastatic melanoma when other treatments do not work or are not safe for you.
Some people have rare types of melanoma. These include mucosal melanoma, acral lentiginous melanoma, and melanoma that spreads to the brain. If you have one of these rare types, you may need special treatments. Chemotherapy can help when other drugs do not work for your metastatic melanoma.
Doctors sometimes use regional chemotherapy, like isolated limb perfusion, for melanoma that stays in one area. This method gives high doses of drugs to the arm or leg. Electrochemotherapy with bleomycin is another option for local treatment. If your metastatic melanoma spreads to the brain, drugs like temozolomide or fotemustine may help.
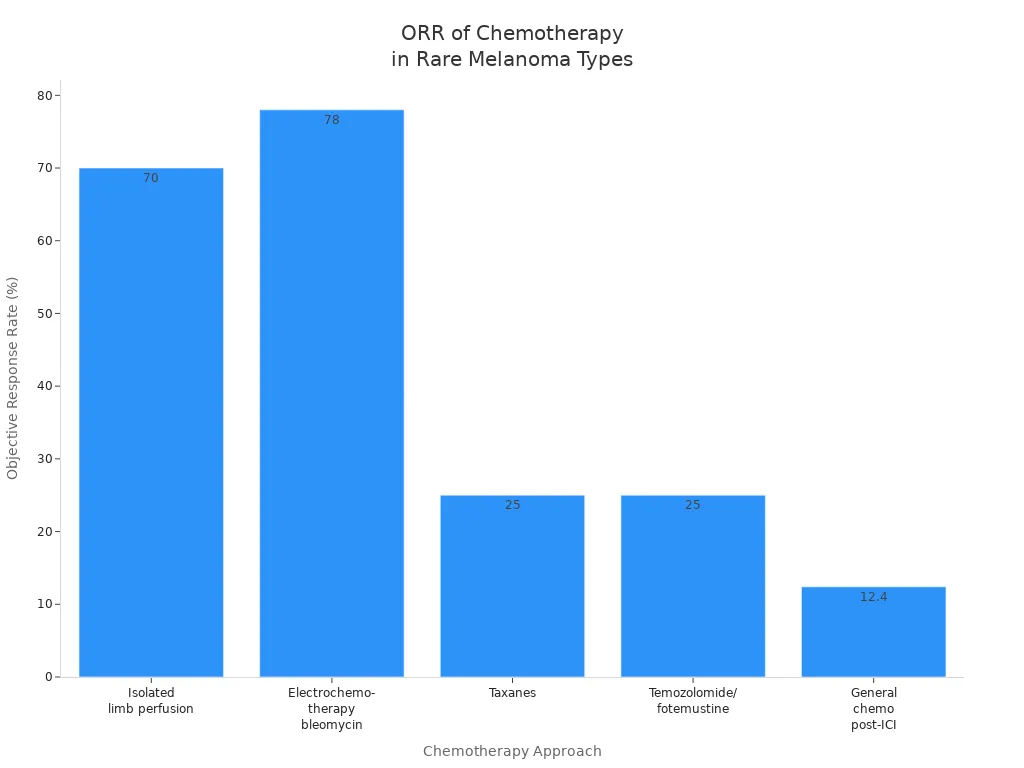
The table below shows how well different chemotherapy approaches work for rare melanoma types:
Chemotherapy Approach | Objective Response Rate (ORR) | Median Overall Survival (OS) | Notes |
|---|---|---|---|
Isolated limb perfusion/infusion | 60–80% | ~40 months | High-dose regional administration for in-transit metastases |
Electrochemotherapy with bleomycin | 78% | N/A | Effective for localized treatment |
Taxanes | 25% | 3.9 months | Highest ORR among chemotherapies post-ICI failure |
Temozolomide/fotemustine | Up to 25% | N/A | Considered for patients with CNS metastases |
General chemotherapy post-ICI failure | 12.4% | 2.6 months | Low activity, not recommended as automatic treatment sequence |
You and your doctor will talk about the best way to treat your metastatic melanoma. Each type of melanoma needs a special plan. Chemotherapy gives you another option when other treatments do not work.
Your doctor might mention chemoimmunotherapy. This means you get chemotherapy and immunotherapy together. Chemotherapy drugs go after melanoma cells. Immunotherapy helps your immune system fight cancer. Using both treatments can help control metastatic melanoma better. Doctors use this mix to make each treatment work harder. You might have more side effects, so your care team will watch you closely.
Chemoradiation is another way to treat metastatic melanoma. You get chemotherapy and radiation at the same time. Radiation targets the melanoma in one area. Chemotherapy makes cancer cells easier to kill with radiation. This mix can shrink tumors and help with symptoms. Doctors use chemoradiation if your melanoma is in one spot or causes pain.
Sometimes doctors use chemotherapy with targeted therapy. Targeted therapy looks for changes in melanoma cells. It blocks signals that help cancer grow. This mix can shrink tumors faster. It works well for some types of metastatic melanoma. Your doctor will check your genes to see if this is right for you.
Combination regimens like carboplatin and paclitaxel are common for metastatic melanoma. This mix has an overall response rate of 11-20% and a median survival of 8.6-11.3 months. BRAF/MEK inhibitor combinations are now the new standard for many patients. These mixes can help you live longer and control your melanoma better.
You have other choices besides chemotherapy drugs. Immunotherapy is a strong treatment for metastatic melanoma. It helps your immune system attack the cancer. Immunotherapy can help 30-40% of people and up to 40% live five years. Chemotherapy, like dacarbazine, works for fewer people and for less time. Immunotherapy usually has fewer side effects than chemotherapy. You may still have immune problems, but they are not the same as chemotherapy side effects.
Targeted therapy is another choice for metastatic melanoma. It focuses on genetic changes in your melanoma. This treatment can shrink tumors fast and keep cancer under control longer. Surgery and radiation are also used for some patients. Surgery removes melanoma in one area. Radiation can shrink tumors and help with pain.
You and your doctor will talk about the best mix or other choice for your metastatic melanoma. Each treatment has its own good and bad points. New research on drugs gives hope for better results.
Chemotherapy drugs for metastatic melanoma are made very carefully. Every step is important for your safety and for the drugs to work well.
Many advanced machines help make chemotherapy drugs. Each one does a special job:
Vial Filling Sealing Line: This machine puts liquid drugs in glass vials and seals them tight.
Prefilled Syringe Filling Line: It gets syringes ready with the right amount of medicine.
Cartridge Filling Line: This fills cartridges that doctors use for some shots.
Ampoule Filling Sealing Line: It puts medicine in small glass ampoules and seals them for one-time use.
Oral Liquid Filling Line: This machine fills bottles with liquid drugs you can drink.
Syrup Filling Line: It works like the oral liquid line but for thicker medicine.
Blow-Fill-Seal (BFS) Machine: This machine makes, fills, and seals containers in one step to keep drugs clean.
Isolator System: It makes a closed, clean space to keep germs away from the drugs.
Pharmaceutical Liquid Preparation System: This mixes and gets the drug solutions ready.
Pharmaceutical Water Treatment System: It cleans the water used to make the drugs.
Other Pharmaceutical Machines: These are mixers, mills, and machines that put labels on.
Tip: All these machines help keep the drugs clean and safe for you.
You want your chemotherapy drugs to be safe and work well. Makers follow strict rules to make sure of this. The FDA and EMA check and approve every drug. Good Manufacturing Practices (GMP) guide each step. Workers test the starting materials, mixtures, and finished drugs many times. They use trusted suppliers and check everything for quality.
A risk assessment helps find and fix problems before you get the drugs. Teams keep making the process better to make drugs safer over time. Sterilization machines, like autoclaves and isolators, kill germs and keep you healthy.
Note: Quality control means you get medicine that works right every time.
If you have metastatic melanoma, you will learn about different chemotherapy drugs. Each drug fights melanoma in its own way. You should know how these drugs work on cancer cells. This helps you understand your treatment.
Alkylating agents are some of the oldest chemotherapy drugs for melanoma. These drugs attack the DNA inside melanoma cells. Damaged DNA stops cells from dividing or growing. This helps stop metastatic melanoma from spreading.
Dacarbazine is the most common alkylating agent for metastatic melanoma. Doctors pick this drug because it slows melanoma growth. You might also hear about temozolomide and lomustine. These drugs work in a similar way.
Note: Alkylating agents can help when other treatments do not work for metastatic melanoma.
Here is a table that shows how dacarbazine helps patients with metastatic melanoma:
Alkylating Agent | Study Type | Patient Group | Progression-Free Survival (PFS) | Overall Survival (OS) |
|---|---|---|---|---|
Dacarbazine (+/− Oblimersen) | Phase III (n=771) | Normal serum LDH | 2.6 months | 11.4 months vs 9.7 months |
Dacarbazine gives patients more time before their melanoma gets worse.
Platinum-based agents are another group of chemotherapy drugs for metastatic melanoma. These drugs have platinum, which is a metal. The drugs stick to DNA in melanoma cells. This stops cells from copying DNA. When cells cannot copy DNA, they die.
Cisplatin and carboplatin are the main platinum-based drugs for metastatic melanoma. Doctors use these drugs alone or with other chemotherapy drugs. Platinum-based agents can shrink tumors and help control symptoms.
Tip: Platinum-based agents are strong drugs. You may need extra care to handle side effects.
Microtubule inhibitors are special chemotherapy drugs. They target microtubules inside melanoma cells. Microtubules help cells divide. When these drugs block microtubules, cells cannot split or grow.
You might get paclitaxel, docetaxel, vinblastine, or vincristine for metastatic melanoma. Paclitaxel and docetaxel make microtubules too stable. Vinblastine and vincristine stop microtubules from forming. Both ways, these drugs stop melanoma cells from spreading.
Here is a table that shows how these drugs work:
Microtubule Inhibitor | Mechanism of Action | Binding Domain |
|---|---|---|
Paclitaxel (PTX) | Promotes tubulin polymerization, causing cell cycle arrest | Taxane binding domain |
Docetaxel (DTX) | Promotes tubulin polymerization, causing cell cycle arrest | Taxane binding domain |
Vinblastine | Inhibits microtubule polymerization | Vinca binding domain |
Vincristine | Inhibits microtubule polymerization | Vinca binding domain |
Vinorelbine | Inhibits microtubule polymerization | Vinca binding domain |
Combretastatin (CA) | Inhibits microtubule polymerization | Colchicine binding domain |
Colchicine | Inhibits microtubule polymerization | Colchicine binding domain |
Paclitaxel has helped some patients with untreated metastatic melanoma. Some people saw their lung tumors shrink for almost a year.
Microtubule inhibitors give you more choices if other chemotherapy drugs do not work for your melanoma.
Antitumor antibiotics are a special group of chemotherapy drugs. These drugs come from natural sources like bacteria. They block enzymes that melanoma cells need to copy DNA. If cells cannot copy DNA, they cannot grow.
Actinomycin D is one example. Doctors do not use this drug often for metastatic melanoma because it can cause more side effects. Sometimes doctors use it in special cases.
Alert: Antitumor antibiotics are very strong. Your doctor will watch you closely if you get these drugs for metastatic melanoma.
You will hear many names when you talk about chemotherapy for metastatic melanoma. Some drugs are used alone. Others are mixed together in regimens. Regimens are plans that use different drugs to fight melanoma in more than one way.
Here is a table with common chemotherapy drugs and their classes:
Drug Name | Drug Class | Main Use in Melanoma |
|---|---|---|
Dacarbazine | Alkylating Agent | Standard for metastatic melanoma |
Temozolomide | Alkylating Agent | Oral option for metastatic melanoma |
Cisplatin | Platinum-Based Agent | Used in combinations |
Carboplatin | Platinum-Based Agent | Used in combinations |
Paclitaxel | Microtubule Inhibitor | Used in regimens |
Vinblastine | Microtubule Inhibitor | Used in regimens |
Actinomycin D | Antitumor Antibiotic | Rarely used |
Doctors often use regimens like:
Carboplatin plus paclitaxel: This is a common choice for metastatic melanoma.
Dacarbazine alone: Used when you need a single drug.
BOLD regimen: Combines bleomycin, vincristine, lomustine, and dacarbazine.
CVD regimen: Uses cisplatin, vinblastine, and dacarbazine.
Dartmouth regimen: Mixes cisplatin, carmustine, dacarbazine, and tamoxifen.
Your doctor will pick the best regimen for your melanoma based on your health and how your metastatic melanoma responds to treatment.
Chemotherapy drugs give you many ways to fight metastatic melanoma. Each drug and regimen has a special job. You and your doctor can work together to find the best plan for your melanoma.
Chemotherapy drugs fight melanoma in different ways. Each drug stops cancer cells from growing or spreading.
Some chemotherapy drugs stop melanoma cells from splitting. These drugs target the cell cycle. The cell cycle is how cells grow and multiply. Paclitaxel and doxorubicin slow down melanoma cell growth. They work based on how much and how long you use them. Some drugs work better together. The table below shows how these treatments change cell growth:
Treatment Type | Effect on Cell Growth | Correlation with CDC25A mRNA Level |
|---|---|---|
Doxorubicin | Inhibited growth in a dose- and time-dependent manner | Negatively correlated |
Paclitaxel | Inhibited growth in a dose- and time-dependent manner | Not correlated |
Combination with NSC663284 | Lower cell viability compared to control or single-drug groups | N/A |
These drugs keep melanoma cells from finishing division. This slows down how fast melanoma spreads.
Some chemotherapy drugs make melanoma cells die. This is called apoptosis. Cisplatin causes damage that cells cannot fix. When this happens, cells stop working or break apart. Here are ways chemotherapy drugs cause cell death:
Cisplatin makes DNA damage. This leads to cell death or stops cell growth.
5-fluorouracil blocks an enzyme called thymidylate synthase. This causes DNA damage and stops the cell cycle.
Some melanoma cells resist these drugs. Researchers look for new ways to make cells die, like necroptosis.
These drugs help shrink melanoma tumors. They do this by killing cancer cells.
Chemotherapy drugs can stop melanoma cells from copying DNA. Without new DNA, cells cannot make new cells. Different drugs use different tricks to block DNA copying. The table below shows how these drugs work:
Mechanism | Description |
|---|---|
DNA Damage | Alkylating agents cause DNA damage, leading to melanoma cell death. |
Methylation Modifications | Methylating drugs create mismatches during DNA copying, causing breaks. |
Crosslinking | Some drugs link DNA strands together, stopping replication and transcription. |
Here is another table that shows how certain drugs block DNA copying:
Drug | Mechanism | Effect |
|---|---|---|
5-Fluorouracil | Inhibits thymidylate synthase | Reduces building blocks for DNA, blocking replication. |
Gemcitabine | Targets ribonucleic acid reductase | Stops cells from making new DNA. |
Cisplatin | Forms DNA crosslinks | Blocks DNA copying, leading to cell death. |
These drugs stop melanoma cells from making more copies. This helps control melanoma growth in your body.
If you know how chemotherapy drugs work, you may feel better about your treatment plan.
When you have metastatic melanoma, you want to know if chemotherapy helps. You also want to see how it compares to other treatments. This section explains how well chemotherapy, immunotherapy, and targeted therapy work. You will learn about response rates and survival outcomes. You will also find out how new drugs and clinical trials change treatment for metastatic melanoma.
Your doctor may talk about response rate. This means how many people see their tumor shrink or stop growing after treatment. In metastatic melanoma, chemotherapy does not work for most people. Clinical trials show only a few patients see their tumors shrink with chemotherapy drugs. Dacarbazine is a main drug. It has a response rate of about 10% to 20%. So, out of 100 people, only 10 to 20 see their tumor get smaller after chemotherapy.
You might get chemotherapy if your melanoma spreads far or if other treatments do not help. Doctors use clinical trials to test new drugs and combinations. Some trials mix chemotherapy with other drugs to try to help more people. The BOLD regimen and CVD regimen use several drugs to fight melanoma cells in different ways. These regimens sometimes help more people in trials, but the benefit does not last long for most.
You may hear about progression-free survival. This means how long you live without your melanoma getting worse. Chemotherapy drugs for metastatic melanoma usually give a short progression-free survival. Most people see their tumors grow again after a few months. Clinical trials show that overall survival with chemotherapy is limited. You may get a few extra months, but the tumor often comes back.
If you join a clinical trial, you may get new drugs that could help more. Ask your doctor about clinical trials for metastatic melanoma.
You have more choices for treating metastatic melanoma now. Immunotherapy and targeted therapy changed how doctors treat melanoma that spreads. These treatments work better for many people, especially if you have a BRAF mutation.
Look at the table below. It shows the two-year overall survival rate for different treatment orders in metastatic melanoma:
Treatment Order | Two-Year Overall Survival Rate |
|---|---|
Immunotherapy first | 72% |
Targeted Therapy first | 52% |
If you get immunotherapy first, you have a better chance to live two years or more. Targeted therapy also helps, especially if your melanoma has a BRAF mutation. Chemotherapy does not give the same survival benefit.
Here is another table that compares overall survival rate and progression-free survival rate for each treatment:
Treatment Type | Overall Survival Rate | Progression-Free Survival Rate |
|---|---|---|
Immunotherapy | 72% | Trending favorably |
Targeted Therapy | 52% | N/A |
Immunotherapy gives you the best chance for long-term survival. Targeted therapy also helps if you have the right mutation. Chemotherapy gives limited overall survival and does not improve progression-free survival for most people with metastatic melanoma.
You can see the clinical benefits of each treatment in the table below:
Treatment Type | Overall Survival Benefit | Progression-Free Survival Benefit |
|---|---|---|
Chemotherapy | Limited | No improvement |
Immunotherapy | Significant improvement | Significant improvement |
Targeted Therapy | N/A | N/A |
You may get chemotherapy if you cannot use immunotherapy or targeted therapy. Some people with rare mutations or special types of metastases may still need chemotherapy. Clinical trials keep testing new drugs to help treat metastatic melanoma.
Talk to your doctor about the best treatment for your melanoma. Ask about your BRAF mutation status, the type of metastases you have, and if you can join clinical trials for new drugs.
You have many choices for treating metastatic melanoma. Immunotherapy and targeted therapy give better survival and response rates for most people. Chemotherapy still helps some, especially if other treatments do not work. New drugs and clinical trials bring hope for better results and longer survival in the future.
Doctors often use intravenous (IV) methods for melanoma. You get medicine through a needle or tube in your vein. The drugs go into your blood fast and start fighting melanoma cells. Nurses watch you closely during IV treatment. You may sit in a special chair at the hospital or clinic. IV methods help many types of melanoma, especially when the cancer has spread.
Some people with melanoma take chemotherapy as pills or capsules. You can swallow these drugs at home. Oral chemotherapy lets you stay comfortable and free. You do not need to go to the hospital as much. But your body may take in the medicine differently each time. You must remember to take your medicine on time. Missing doses can make melanoma harder to treat.
Chemotherapy for melanoma usually follows a cycle. You take the drugs for a set number of days, then rest. This pattern helps your body recover between treatments. Your doctor will tell you how many cycles you need. The number depends on how your melanoma responds. You may feel tired or have other side effects during each cycle. Common side effects are fatigue, hair loss, nausea, vomiting, low blood count, mouth sores, and skin rash.
Here is a table that shows the main ways to get chemotherapy for melanoma:
Method of Administration | Advantages | Disadvantages |
|---|---|---|
Intravenous (IV) | Rapid delivery to the bloodstream | Requires medical supervision |
Oral | Convenient and can be taken at home | Variable absorption rates |
Combination Therapy | Increases effectiveness against cancer cells | Higher risk of side effects |
Tip: Always talk to your doctor if you have questions about your melanoma treatment plan.
When you get chemotherapy for melanoma, your body may change. These drugs fight melanoma cells, but they can hurt healthy cells too. You might feel tired or weak. Some people lose hair or feel sick. Others get mouth sores or nail changes. Your skin may get dry or itchy. You could bruise or bleed more because your blood cell count drops.
Doctors watch for side effects to keep you safe. The table below lists common problems people have during melanoma treatment:
Chemotherapy Drug | Common Grade 3/4 Adverse Events |
|---|---|
General | Neutropenia, Vomiting, Anemia |
Vemurafenib | Cutaneous squamous-cell carcinoma, Rash, Elevated liver enzymes |
Dabrafenib | Cutaneous squamous-cell carcinoma, Pyrexia |
Trametinib | Hypertension, Rash |
Ipilimumab | Immune-related diarrhea/colitis, Dyspnea, Anemia, Vomiting, Hypophysitis |
Talimogene laherparepvec | Cellulitis |
You may feel numbness in your hands or feet. Some people notice changes in vision or hearing. Always tell your doctor about new symptoms. Your safety is very important during melanoma treatment.
You can do things to help with side effects from chemotherapy. Drink lots of water to help your body. Eat small meals if you feel sick. Rest when you are tired. Use gentle shampoo if you lose hair. Wear sunscreen to protect your skin, since melanoma and its treatment can make you more sensitive to sunlight.
Doctors may give you medicine for nausea or to help you sleep. Nurses check your blood often to keep you safe. If you get a fever or chills, call your doctor right away. Quick action helps keep you safe.
Tip: Write down your symptoms in a diary. This helps your care team change your melanoma treatment for better safety and comfort.
You help keep yourself safe. Stay in touch with your care team and ask questions about your melanoma treatment. By working together, you can handle side effects and focus on getting better.
You might wonder when doctors use chemotherapy drugs for metastatic melanoma. Most people start with immunotherapy or targeted therapy. These treatments help many patients. If these do not work, your doctor may suggest chemotherapy. Sometimes, you cannot get immunotherapy or targeted therapy because of other health issues. In those cases, chemotherapy is important.
Doctors check your melanoma type and your health before making a plan. If you have a BRAF mutation, you may get targeted therapy first. If you do not have this mutation, immunotherapy is usually the first choice. Chemotherapy is used when other treatments do not help or if your melanoma grows fast.
Here is a table that shows common treatment choices for different types of metastatic melanoma:
Patient Type | Recommended Treatments |
|---|---|
BRAF Wild-Type, Unresectable/Metastatic Melanoma | Nivolumab + Ipilimumab, Nivolumab + Relatlimab, Nivolumab, Pembrolizumab |
BRAF Mutant (V600), Unresectable/Metastatic Melanoma | Nivolumab + Ipilimumab, Nivolumab + Relatlimab, Nivolumab, Pembrolizumab, Dabrafenib + Trametinib, Encorafenib + Binimetinib, Vemurafenib + Cobimetinib |
New Recommendation (2023) | Nivolumab + Relatlimab based on RELATIVITY-047 trial results |
Doctors use chemotherapy for metastatic melanoma when other treatments do not work or are not safe for you.
Some people have rare types of melanoma. These include mucosal melanoma, acral lentiginous melanoma, and melanoma that spreads to the brain. If you have one of these rare types, you may need special treatments. Chemotherapy can help when other drugs do not work for your metastatic melanoma.
Doctors sometimes use regional chemotherapy, like isolated limb perfusion, for melanoma that stays in one area. This method gives high doses of drugs to the arm or leg. Electrochemotherapy with bleomycin is another option for local treatment. If your metastatic melanoma spreads to the brain, drugs like temozolomide or fotemustine may help.
The table below shows how well different chemotherapy approaches work for rare melanoma types:
Chemotherapy Approach | Objective Response Rate (ORR) | Median Overall Survival (OS) | Notes |
|---|---|---|---|
Isolated limb perfusion/infusion | 60–80% | ~40 months | High-dose regional administration for in-transit metastases |
Electrochemotherapy with bleomycin | 78% | N/A | Effective for localized treatment |
Taxanes | 25% | 3.9 months | Highest ORR among chemotherapies post-ICI failure |
Temozolomide/fotemustine | Up to 25% | N/A | Considered for patients with CNS metastases |
General chemotherapy post-ICI failure | 12.4% | 2.6 months | Low activity, not recommended as automatic treatment sequence |
You and your doctor will talk about the best way to treat your metastatic melanoma. Each type of melanoma needs a special plan. Chemotherapy gives you another option when other treatments do not work.
Your doctor might mention chemoimmunotherapy. This means you get chemotherapy and immunotherapy together. Chemotherapy drugs go after melanoma cells. Immunotherapy helps your immune system fight cancer. Using both treatments can help control metastatic melanoma better. Doctors use this mix to make each treatment work harder. You might have more side effects, so your care team will watch you closely.
Chemoradiation is another way to treat metastatic melanoma. You get chemotherapy and radiation at the same time. Radiation targets the melanoma in one area. Chemotherapy makes cancer cells easier to kill with radiation. This mix can shrink tumors and help with symptoms. Doctors use chemoradiation if your melanoma is in one spot or causes pain.
Sometimes doctors use chemotherapy with targeted therapy. Targeted therapy looks for changes in melanoma cells. It blocks signals that help cancer grow. This mix can shrink tumors faster. It works well for some types of metastatic melanoma. Your doctor will check your genes to see if this is right for you.
Combination regimens like carboplatin and paclitaxel are common for metastatic melanoma. This mix has an overall response rate of 11-20% and a median survival of 8.6-11.3 months. BRAF/MEK inhibitor combinations are now the new standard for many patients. These mixes can help you live longer and control your melanoma better.
You have other choices besides chemotherapy drugs. Immunotherapy is a strong treatment for metastatic melanoma. It helps your immune system attack the cancer. Immunotherapy can help 30-40% of people and up to 40% live five years. Chemotherapy, like dacarbazine, works for fewer people and for less time. Immunotherapy usually has fewer side effects than chemotherapy. You may still have immune problems, but they are not the same as chemotherapy side effects.
Targeted therapy is another choice for metastatic melanoma. It focuses on genetic changes in your melanoma. This treatment can shrink tumors fast and keep cancer under control longer. Surgery and radiation are also used for some patients. Surgery removes melanoma in one area. Radiation can shrink tumors and help with pain.
You and your doctor will talk about the best mix or other choice for your metastatic melanoma. Each treatment has its own good and bad points. New research on drugs gives hope for better results.
You may wonder how companies keep chemotherapy drugs safe. Special machines and tools help protect you and the workers. These machines are very important in making the drugs:
Containment Facilities: These buildings hold strong drug ingredients inside. They stop them from getting out.
Isolators and Restricted Access Barrier Systems (RABS): These machines let workers handle drugs without touching them. They keep out germs and dust.
Single-Use Technologies (SUTs): These are bags, filters, and bioreactors used one time. They help stop germs from spreading.
High-Efficiency Particulate Air (HEPA) Filtration: These filters clean the air. They keep bad particles away from the drugs.
Automation and Robotics: Robots and machines do many jobs. They fill bottles, seal vials, and move drugs.
Ventilated Biological Safety Cabinets: These cabinets keep workers safe when they prepare chemotherapy drugs.
Personal Protective Equipment (PPE): Workers wear gloves, gowns, and masks to stay safe.
Closed System Transfer Devices: These tools move drugs between containers. They stop anything from leaking out.
Needle-Free Devices: These tools help stop needle injuries. They also keep the drugs clean.
Using these machines and tools helps make sure your medicine is always clean and safe.
You want your chemotherapy drugs to be clean and safe. Drug makers use special steps to keep everything free from germs. They also check the quality at every step. Here is a table that shows how they do this:
Sterilization Process | Description |
|---|---|
Aseptic Vial Filling | Vials are filled in a clean space. They are washed, dried, and sealed to stop germs from getting in. |
Lyophilization | This process takes water out of drugs. It makes a dry powder that lasts longer and stays stable. |
Pharmaceutical Autoclave | This machine uses heat and steam to clean vials and tools. It kills all germs and keeps things safe. |
Quality control teams test the drugs at every step. They check the amount of medicine and look for germs. They make sure nothing is missing. You can trust that each dose follows strict safety rules before you get it.
Tip: Clean machines and careful checks keep you healthy and help your treatment work well.
When you start treatment for metastatic melanoma, you need to talk openly with your doctor. Asking the right questions helps you understand your options and feel more confident about your care. You can use these questions to guide your conversation.
Here are important questions you should ask your doctor about chemotherapy drugs:
How much experience do you have treating this type of cancer?
What are my treatment options? What are the possible risks and benefits of each?
Which treatment do you recommend? Why?
What is the main goal of this treatment?
Should I get a second opinion? Can you suggest another doctor or cancer center?
How soon do I need to decide on treatment?
How should I prepare for chemotherapy?
How long will treatment last? What will it be like? Where will I get it?
What side effects should I expect? How long might they last?
Will treatment affect my daily activities?
What are the chances of my cancer coming back with these drugs? What happens if it does?
How will we know if the treatment is working?
What can I do to help manage side effects?
What symptoms should I tell you about right away?
How can I reach you or your team after hours?
Are there any limits on what I can do during treatment?
Do you know of any support groups or mental health professionals I can talk to?
Tip: Write down your questions before your visit. Bring a notebook to keep track of answers.
You need to understand both the risks and benefits of chemotherapy drugs for metastatic melanoma. Chemotherapy can help control symptoms and may slow the growth of cancer. Some people find that single drugs are easier to tolerate. Combination therapies can sometimes cause more side effects without improving survival rates. You should talk with your doctor about what you can expect from each option.
Chemotherapy drugs can cause unwanted effects in other parts of your body. You might need regular checkups to watch for these problems. Your doctor may adjust your treatment if you have strong side effects. Always tell your care team about any new symptoms. This helps them keep you safe and comfortable during treatment.
Note: Regular monitoring and honest talks with your doctor help you get the best care possible.
You have lots of ways to treat metastatic melanoma. Chemotherapy drugs like dacarbazine and carboplatin are still used. New treatments for melanoma give people more hope. The table below shows how chemotherapy helps with metastatic melanoma:
Study Type | Chemotherapy Regimen | Overall Response Rate | Disease Control Rate |
|---|---|---|---|
Phase II | Investigator-choice chemotherapy | 4% | 22% |
Phase III | Dacarbazine or carboplatin plus paclitaxel | 11% | 45% |
Immunotherapy has changed how doctors treat melanoma. It helps many people with metastatic melanoma. You should talk to your doctor about every treatment choice. Your care team will help you pick the best plan for your melanoma. New treatments for metastatic melanoma give you more hope for the future.
Metastatic melanoma happens when melanoma spreads past your skin. It can move to places like your lungs, liver, brain, or bones. Doctors use special treatments to fight melanoma in these spots.
Chemotherapy drugs go after melanoma cells and stop them from growing. You might get these drugs if other treatments do not help. Your doctor picks the best drug for your melanoma. Chemotherapy can make tumors smaller and help with symptoms.
You might feel tired, lose your hair, or feel sick to your stomach. Some people see changes in their skin or nails. Chemotherapy can lower your blood cell count. Your doctor checks on you to help with side effects from melanoma treatment.
Doctors use chemotherapy if immunotherapy or targeted therapy does not work. You may need chemotherapy if your melanoma grows fast or spreads to rare places. Some types of melanoma do better with chemotherapy than others.
You can use chemotherapy with immunotherapy, radiation, or targeted therapy. This mix helps control melanoma and may work better. Your doctor chooses the best plan for your melanoma. Using more than one treatment gives you more ways to fight melanoma.